Turns out this is true for farmers building baseball diamonds in fields to attract ghosts. But sadly it is not true for providers trying to get patients into their practice.
Patient engagement is a case where simply setting up shop isn’t enough. You have to put in lots of work, at every phase of the journey if you want a chance of being successful.
A quick online search for “Patient Engagement Companies” returns 100’s of results. There are entirely new companies focused on this space, along with every major player and big name trying to grab a piece of the market.
It’s a space where so much can be done and is being done. There’s lots of time and resources being spent without a lot of results. It seems like we are mistaking activity on its own as the answer rather than stepping back and examining if we are actually tackling the problems and working from first principles. Or we are going to the other extreme and doing nothing, and just expecting patients to show up.
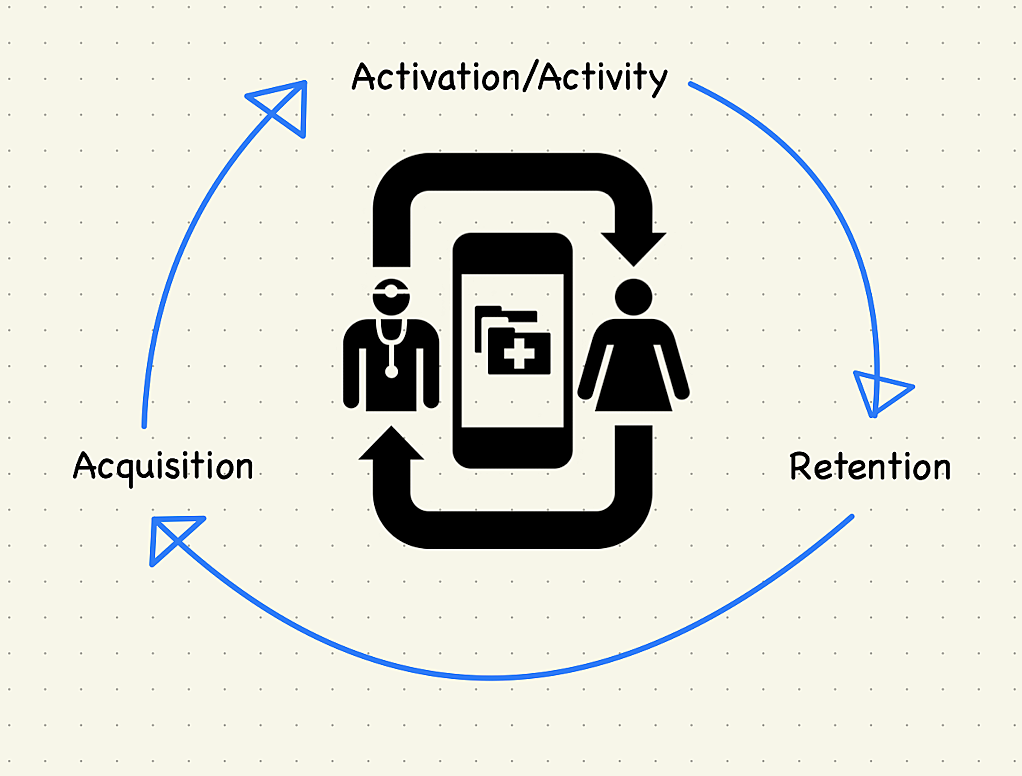
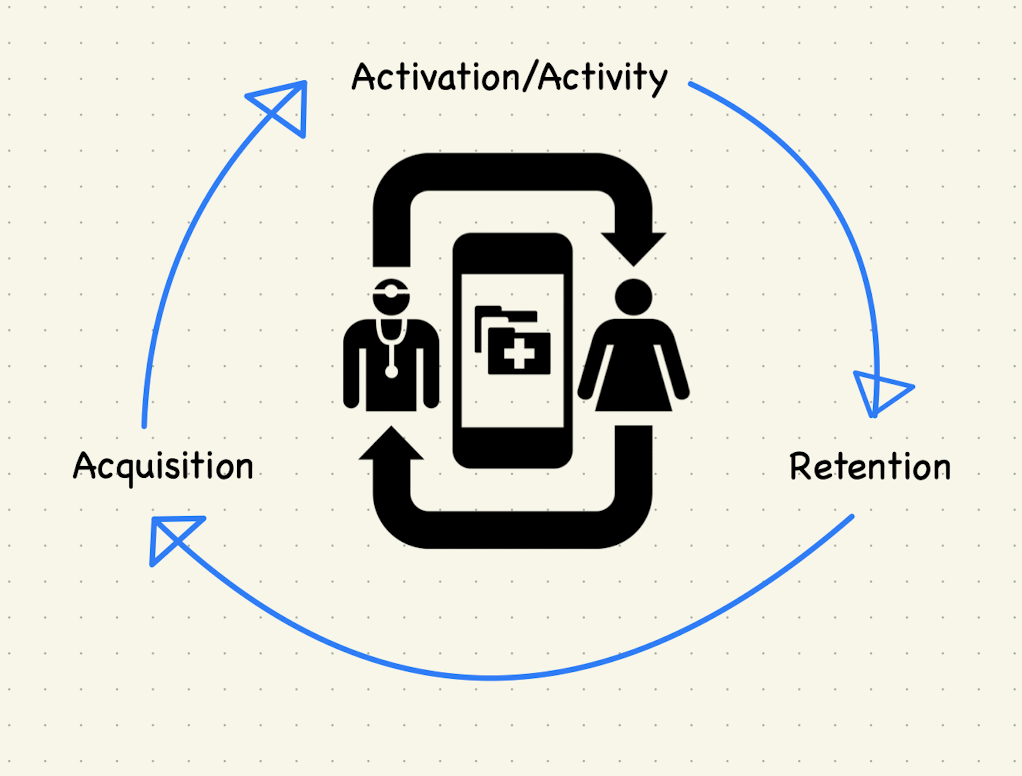
This is my attempt to frame out the basic steps of the patient engagement cycle, to give some structure to how we can engage patients, improve their health and succeed financially. This is not meant to be an exhaustive look at all things patient engagement. Or a deep dive into every unique tactic out there. There are multiple companies attacking each piece of this landscape, I’ll leave the deep work to them. This is a way to prioritize your efforts and align your resources.
(Pro tip: when trying to bring clarity to a subject nothing works better then putting an image of a cycle inside another cycle)
Acquisition
This is where everything starts. Before you can engage patients you need patients to engage. And even once you have patients you will need to continue growing your panel.
In this phase I see a couple things as being paramount: Demonstrating Value to Payers, Building Trust, and Establishing Your Reputation. Doing these things correctly will position you to gain patient share in an increasingly competitive environment. Let’s take a deeper look at each:
Ultimately payers are going to be your biggest source of patients. They have the member populations and the power to assign them to your panel. Getting aligned with them is key to long-term success and growth.
There are many ways to demonstrate your value to payers, each deserves a deeper, technical dive but for now we’ll stay high level.
Current Results: be able to show success with current patients. This comes in the form of both health/quality outcomes and financial success. Payers want to make sure you can give the proper care to their members in a cost effective way.
Be a Partner: Instead of just taking the standard contract from the payer look at options to partner. Are there ways to can get creative together? Perhaps taking more risk on to get a larger population of patients added to your panel? Show them that you are willing to be flexible and work together to get to the best outcomes for everyone.
Outside of payers assigning patients to you, another major stream of patients will be through referrals and word of mouth. You need to be someone to whom other providers will send their patients. And you need to be the first name that comes to mind when a patient’s friend or family asks them for a good provider.
Anecdotally, I’ve had several PCPs in my life and had quite a few specialist visits. All of them were sourced through word of mouth. I may be somewhat unique in that experience but I definitely think I’m much more rule than exception.
Activation/Activity
This is where things get tough. This is the phase that can make or break you. It’s challenging because you have to get people to take action. And not just take any action but the right action at the right time.
There are a number of things to focus on here, including: Establishing a Baseline Health Status, Addressing Care Gaps, Utilizing Incentives, and Educating Patients. This list could be much longer but this gives us a good start.
Establish a Baseline Health Status
Ideally you would do this at the population, sub-population and individual patient levels. But that is much easier said than done. In theory this should be easy; payers should be able to provide you with all the needed information. But between data quality, differing formats and interchange issues; this option becomes slow or grinds to a halt. So it’s often on the provider to gather updated information on each patient.
Doing this in person is challenging in a world where 1000’s of patients can be assigned to a panel. The physical provider to patient interaction can’t scale to meet those types of numbers. (In theory telehealth was supposed to help here. But telehealth in its current iteration is just a digital twin of the in office experience. Rather than bringing real benefits of scale and technology it just changes where care takes place.)
Another route is to try and gather this information from patients digitally through marketing, surveys and apps. All have a role to play but response/use rates aren’t great with any of these.
To make this piece work currently you have to use all of the above, with lots of manual effort, to try and gather an understanding of just how healthy/sick your patients are currently.
Once you have that baseline it’s time to help those who are sickest or most at risk.
Again this is challenging because patients may not be aware there is an issue or may not be as concerned as you are about it.
This is another place where there is lots of manual work to be done: verifying that gaps exist, trying to get a hold of patients, and trying to get them to take the steps necessary to close the gaps.
Utilizing Incentives
One common practice for getting patients to act is using incentives An example here, my previous insurance carrier would give me (and each member of my family) a $100 gift card for getting my flu shot.
Incentives seem to be one area where a lot of trial and creativity is happening. Trying to determine what actually matters to patients and what will get them engaged.
Hand in hand with using incentives is managing the risks around them. If not structured correctly you could find yourself incentivizing the wrong behaviors or spending more than is cost effective. Back to the example of flu shots, in the case of my family we were going to get the flu shot regardless of the incentive. So that means our insurance company spent $400 more than was needed for us to take action. And speaking of mis-incentives we are now expecting that incentive for doing something routine. So next year we may wait to get the shot or not get it at all until we know the gift cards are coming.
This is a low stakes example but as you work to incentivize bigger populations of sicker patients you have to ensure that the incentives work (people take action) but that the financial numbers also work out on the backend.
Lots to be said here, entire industries and professions exist in this space. But the upshot here is making sure that patients have the information they need to make appropriate care decisions. And ensuring they are aware of their options.
A classic example here is in educating patients on when to visit an Urgent Care vs ED. For someone who came up in healthcare I used to see this as trivial. It was obvious what each facility was designed to do. But as I started working with patients I saw this really was a knowledge gap. A gap with potentially massive health and financial implications.
Once patients know what type of care is appropriate we also need to let them know their options for receiving that care. Another anecdote here, my PCP sent me an email a while back letting me know they had opened an urgent care. But more importantly they would waive the copay for any urgent care visits done through telehealth. I’ve since taken advantage of this benefit a few times. It even got me to see a provider in times where I would have tried to just ride out being sick or injured. Letting me know of this option meant better outcomes for both myself and my provider.
Retention
Say you do all of the above right, you still have one more challenging phase to get through. Once you’ve gathered patients and cared for them, you’ve got to convince them to stay (either directly or indirectly). Depending on the patient type, you may be trying to retain then directly or you may be facing the task of convincing their payer/employer to let you keep them. Again way too much to unpack here but two things that I find really interesting in this space: Outcomes Analytics and Direct Primary Care.
As I mentioned, payers usually have all the data you need about your patients. The challenge is getting that data. Getting everything you need, in a format you can use and in a timely manner. Instead of relying solely on the payers and their data, you should be working to build your own analytics program.
Depending on your size and expertise this could look like buying an off the shelf product from a number of vendors. Or if you are bigger with more budget and more in-house expertise you can build your own analytics packages.
However you do it, it’s critical to have the data and ability to show the outcomes of all your efforts.
One interesting option for providers is to avoid payers all together and go straight to patients. This applies both to new patients and to currently insured patients.
DPC can be used as an option to provide care to patients who are not insured and would otherwise not become patients. These DPC arraignments are usually built on a subscriber model. This means that the provider gets a new stream of recurring revenue. And the patient gets the care they need.
Additionally, I have seen providers offering a DPC option to patients whose insurance changes. When a patient’s insurer changes and their provider is no longer in-network, that patient usually has to find a new provider. But a DPC option means that a patient can decide to maintain the relationship with their provider in exchange for an out-of-pocket cost.
In my mind, framing engagement in these 3 phases gives you a great foundation for success. But I also spent a lot of time unpacking challenges and issues that exist at each phase. Unfortunately I don’t have answers for how to address all of those. Luckily, we’re in a time of great innovation in this area. There are opportunities for providers both big and small to succeed. There are solutions out there, both full stack for those who wants something that can just go from day one. Or for those looking for custom work all the building blocks are readily available. Hopefully this gets you thinking. And I would love to hear from experts who can tell me what I got wrong and help me see my blind spots on the subject.